THERAPEUTIC AREA
Immunooncology
DEVELOPMENT STAGE
Phase I Clinical Trial
ENROLLMENT
Started Dec 2024
SEEKING
Licensing · Co-development
PHASE I KEY FINDINGS
Early Clinical Data Confirms the Hypothesis
0 DLT
No dose-limiting toxicity across 6 cohorts (0.01–3.0 mg/kg)
5/6
Evaluable subjects confirmed immune reservoir mobilization, first detected at 0.03 mg/kg
3/5
Evaluable subjects achieved disease control — including 6-month SD in colon cancer, exceeding all approved 3L mCRC standards
THE CHALLENGE
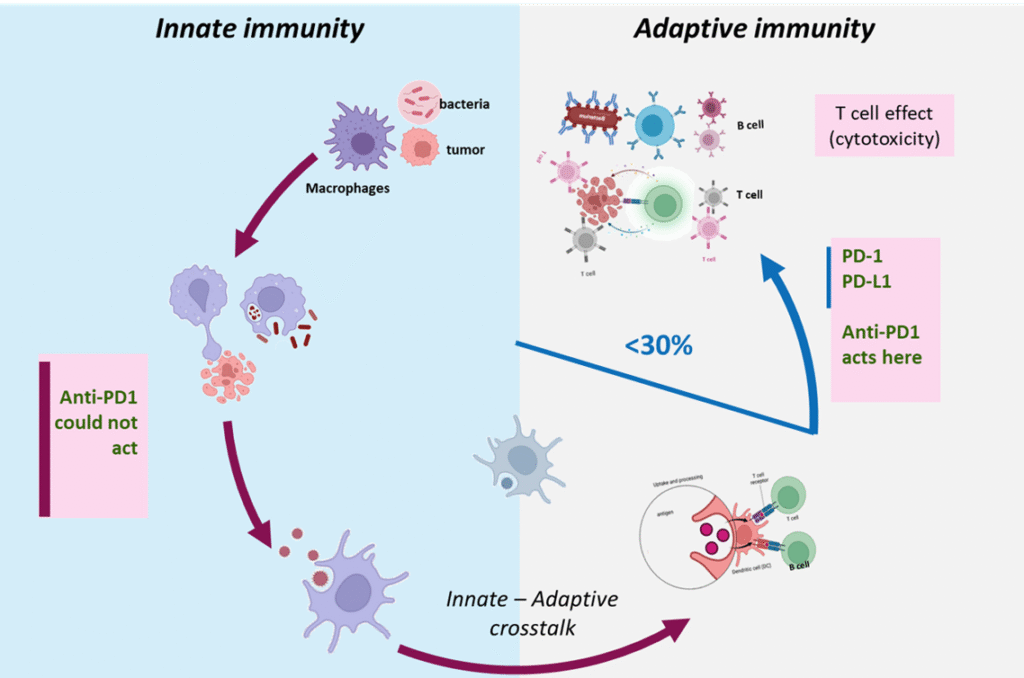
Why Current Immunotherapies Fall Short
Less than 30% of cancer patients respond to anti-PD-1. The reason: most tumors suppress immunity upstream of PD-1, at the innate immune level — where existing therapies cannot reach.
“Releasing the wrong brake doesn’t move the car. The bottleneck is upstream.”
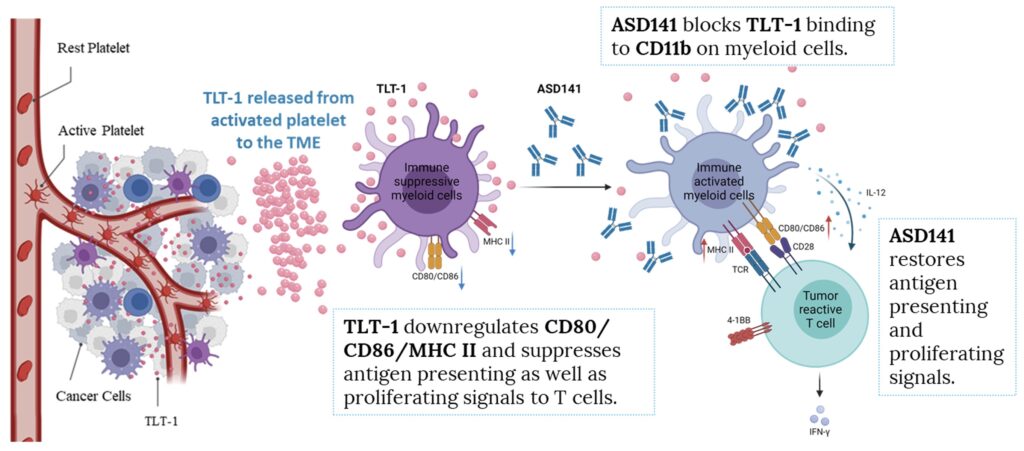
THE SOLUTION
Targeting the Root of Immune Suppression
ASD141 blocks TLT-1/CD11b signaling, dismantling immune suppression at its source and mobilizing self-renewing T cells to restore anti-tumor immunity.
In preclinical humanized mouse models, ASD141 demonstrated anti-tumor activity as monotherapy and synergistic effects when combined with anti-PD-1 or anti-CTLA-4 — without additive toxicity.
MECHANISM OF ACTION
ASD141 Conquers the Dual Barrier
To address the 70% gap in immunotherapy response, ASD141 targets two distinct barriers simultaneously.
BARRIER 1
Checkpoint Barrier
Remodels the tumor microenvironment in PD-1 refractory tumors by blocking TLT-1/CD11b immune suppression at its source.
BARRIER 2
Regenerative Barrier
Mobilizes stem-like TCF-1⁺PD-1⁺CD8⁺ T cells from the immune reservoir, restoring productive anti-tumor immunity — confirmed in all evaluable Phase I subjects.
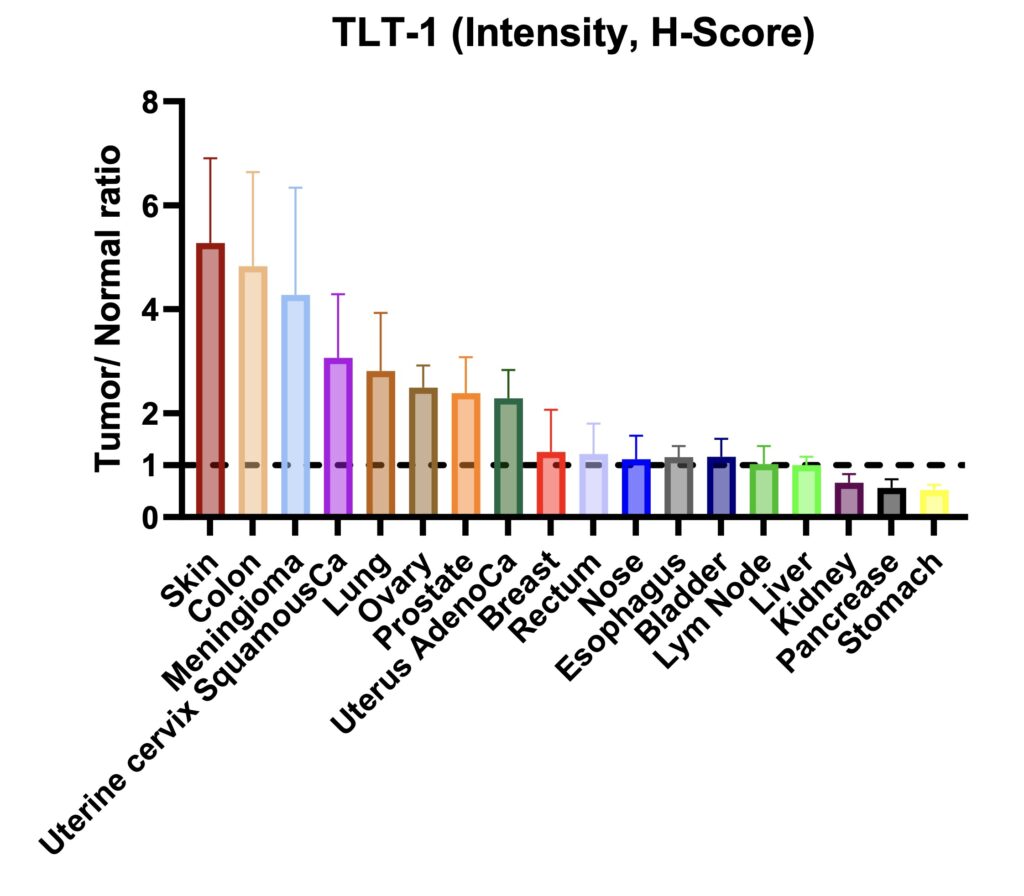
BIOMARKER
Patient Selection with TLT-1
Tumors overexpressing TLT-1 are largely refractory to anti-PD-1 — defining a biomarker-selected population for ASD141.
Highest expression confirmed in ovarian, uterine, prostate, colon, and cervical cancers. Two validated biomarkers support a de-risked, enrichment-driven development strategy.
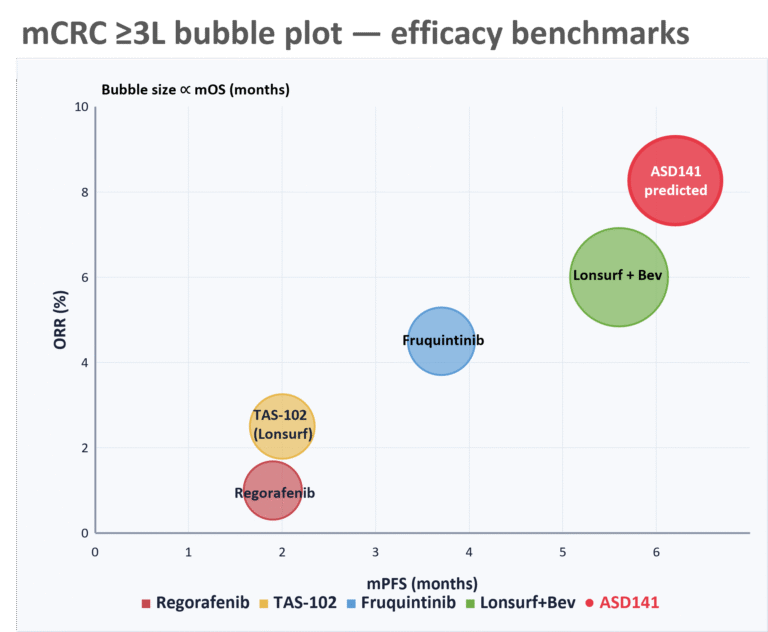
COMPETITIVE POSITION
Potential to Outperforming the Standard of Care
ASD141’s first 3L+ colon cancer patient achieved ≥6 months stable disease — already exceeding the historical mPFS of every approved 3L mCRC option.
Combined addressable market in mCRC and platinum-resistant ovarian cancer: ~$9.5B today, scaling toward $25B+.
Restores Innate Immune Activity
Reactivates suppressed myeloid cells within the tumor microenvironment to coordinate an anti-tumor response.
Bridges Innate and Adaptive Immunity
Enhances innate-adaptive immune signaling, enabling a more comprehensive immune attack.

Drives Antigen Presentation
Promotes active antigen-presenting cells into the tumor environment, priming downstream T cell responses.
Ready to Explore a Partnership?
Our business development team is available for confidential discussions on licensing, co-development, and investment opportunities.
References
1. Schoenfeld AJ, Hellmann MD. Acquired resistance to immune checkpoint inhibitors. Cancer Cell. 2020;37(4):443-455.
2. Haslam A, Prasad V. JAMA Netw Open. 2019;2(5):e192535.
3. Ascendo unpublished data.
4. Shimabukuro-Vornhagen A et al. J Immunother Cancer. 2018;6(1):56.
5. Tay SH et al. Front Immunol. 2022;13:807050.
6. Bertrand A et al. BMC Med. 2015;13:211.
7. Chen X, Song E. Cancer Commun. 2022.